|
||||||||
|
||||||||
|
|
The shoulder is a very elegant and complex piece of machinery. The design of
the shoulder gives us the ability to do useful things by helping us to
reach and use our hands in many different positions. This design gives
the shoulder joint a great range of motion but not much stability.
An
injury to these tendons can result in a weak painful, shoulder. Let's
look at how this can occur.
WHAT DO YOU FEEL with cuff problems?
Early
symptoms of rotator cuff problems include generalized aching of the
shoulder and pain when raising the arm out from the body. Most patients
complain of difficulty sleeping due to pain, especially when they roll
over on the affected shoulder. A reliable sign of impingement is
a sharp pain when trying to reach into your back pocket.
As the
process continues, discomfort increases and the joint may become
stiffer. Sometimes a "catching" sensation is felt when the arm is
lowered. Weakness and inability to raise the arm, as well as severe
night pain, may indicate that the rotator cuff tendons are actually
torn.
WHAT IS
THE ROTATOR CUFF?
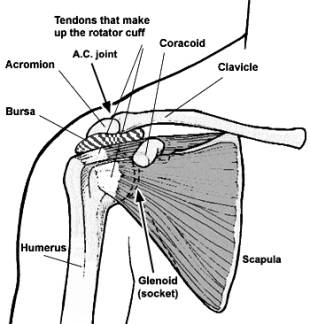
The
shoulder is made of three bones: the scapula (shoulder blade), the
humerus (upper arm bone) and the clavicle (collarbone). The
shoulder is a ball and socket joint similar to the hip, although
in the shoulder, the socket is very shallow and has an appearance
similar to that of a golf ball on a golf tee. In order to gain
stability, the shoulder has specific muscles that keep the ball centered
in the socket.
The
tendons of these muscles (called the supraspinatus,
infraspinatus, teres minor, and subscapularis) form
the rotator cuff. Tendons attach muscles to bones, allowing the muscles
to pull and produce motion. The rotator cuff complex connects the
humerus with the scapula (shoulder blade) and helps stabilize and rotate
as the arm is raised by the deltoid (the outer layer of muscle). The
rotator cuff holds the ball of the humerus tightly in the socket (glenoid)
of the scapula. The part of the scapula that makes up the roof of the shoulder, and serves as the origin for the deltoid, is called the acromion. Between the acromion and the rotator cuff, there is a bursa. A bursa is a lubricated sac of tissue that protects the muscles and tendons as they move against one another. The bursa simply allows the moving parts to slide against one another without too much friction. Treating an inflamed bursa alone will not fix the underlying problem.
Without
function of the rotator cuff, the deltoid will pull the humeral head
upwards to rub against the acromion, irritating the bursa, and even
eventually tearing the tendons of the cuff itself. WHAT
IS A ROTATOR CUFF TENDINITIS or shoulder impingement?
Shoulder
impingement is the pinching of a tendon or bursa between the acromion
and the humeral head. This can be caused by:
·
Anatomy
- The actual shape of the bones in your shoulder or the presence of a
bone spur in the shoulder may cause an impingement
·
Weak
muscles - The muscles in your shoulder (the rotator cuff) and in your
mid-back (called the scapular stabilizers) can cause improper movement
of the shoulder, producing pinching of the tendons and bursa.
·
Shoulder
instability - Instability at the shoulder joint may also cause shoulder
impingement symptoms.
Usually,
there is enough room between the acromion and the rotator cuff so that
the tendons slide easily underneath the acromion as the arm is raised.
But each time the arm is raised, rubbing does occur. This rubbing, or
pinching action, is called impingement. Impingement occurs to
some degree in everyone’s shoulder, caused by day to day activities that
we do with the arm above shoulder level.
But
continuously working with the arms raised overhead, repeated throwing
activities, or other repetitive actions of the arm can cause impingement
to become a problem.
Irritation of the bursa and rotator cuff tendons comes in a wide
spectrum and has many names. All of these names refer to different
degrees of the disease process, but are not necessarily separate items.
For example, the terms rotator cuff syndrome,
shoulder bursitis, rotator cuff tendinitis, and
impingement syndrome all refer to the same thing. The next
step in the disease process would be a partial thickness
rotator cuff tear. The final step in the disease process
would be a full thickness rotator cuff tear.
(see the figures on the next page)
How can
I prevent this injury from recurring?
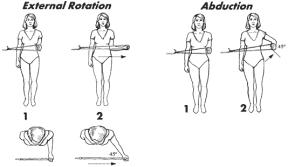
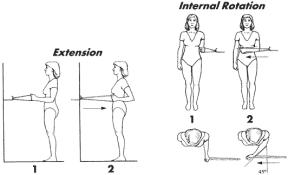
The best
way is through daily shoulder exercises. Do not work through sharp pain
when performing exercise or activities of daily living. If you are
experiencing sharp pain with an exercise or activity, you should stop
and inform your doctor or physical therapist. They will both help
educate you to prevent this injury from recurring.
WHO GETS
ROTATOR CUFF Tendinitis
and TEARS? Rotator cuff tendinitis can be either a wear and tear process that starts gradually without any evidence of an injury, or it can follow an acute event such as a fall or when lifting and twisting in an unusual position. While it is most common between the ages of 40 and 60, it may start as early as one’s 20s or present as late as one’s 80s. It happens in both men and women. Can you
DIFFERENTIATE tendinitis Versus a partial tear
versus a full-thickness cuff tear by history and physical
exam alone? No. A torn rotator cuff commonly causes weakness and pain in the shoulder, although many patients with known tears of the rotator cuff have surprisingly few symptoms. Unless there is clearly no strength with lifting the arm or with rotating it outward, it is often impossible to tell the difference between tendinitis and a cuff tear. What
imaging studies are used to see the cuff? X-rays do not show evidence of rotator cuff tears, unless the tear is so old and so large that bony changes have occurred. If such changes are seen, it generally predicts a poor outcome. An MRI scan or arthrogram is the next step if there is a suspected tear of the rotator cuff tendons. An MRI scan is a special radiological test where magnetic waves are used to create pictures that look like slices of the shoulder. The MRI scan shows soft tissues like tendons and ligaments better than it does bones. The MRI scan is painless, and requires no needles or dye to be injected. The arthrogram is an older test, done by injecting dye into the shoulder joint and taking several X-rays. If the dye leaks out of the shoulder joint, it suggests that there is a tear in the rotator cuff tendons. Both tests are still widely used. Many physicians consider them to be ‘pre-operative’ studies, only ordered if surgical treatment is being considered. What
causes actual tears of the rotator cuff? Many studies have shown that the rotator cuff tendons have areas where there is a very poor blood supply. In the human body, the better the blood supply a tissue has, the better and faster that tissue can repair and maintain itself from day to day wear and tear. These areas of poor blood supply in the tendon make the rotator cuff tendons especially vulnerable to degeneration with aging. This simple condition of aging may help explain why the rotator cuff tear is fairly common in later life. Rotator cuff tears usually occur through areas of the tendon that were not normal to begin with and have been weakened by degeneration and impingement.
Rotator
cuff tears can be either of gradual onset or can occur because of an
injury. The most common type of rotator cuff tear, a chronic tear, is an
attritional process. Over time, the rotator cuff rubs back and forth
against the underside of the acromion, which gradually tears fibers of
the rotator cuff. Eventually a full thickness tear is present and may
cause pain not only with activity, but also at rest. The other type of
rotator cuff tear is a traumatic tear that may occur following a fall, a
dislocation, or other high energy injury to the arm.
Typically, a rotator cuff tear occurs in a late middle-aged person who
has been having problems with the shoulder for some time before the
acute event. That person starts a lifting activity that exceeds the
strength of the tendons, and the tendon tears, leaving an inability to
raise the arm. There may be, or may not be, pain associated with the
event.
Not all
rotator cuff tears are repairable. Sometimes, the tendon has been torn
for too long. This can lead to the tendon and muscle contracting.
The muscle and tendon cannot be stretched enough to be attached back to
where it was torn from. In other cases, the tendon tissue has simply
worn away, and what tendon remains is not strong enough to hold the
stitches necessary to attach the tendon to bone. In these circumstances,
simply removing all the torn tissue and fixing any other problems in the
shoulder (such as acromioclavicular (AC) joint arthrosis and impingement
syndrome) may reduce pain. It will probably not increase the
strength or motion of the shoulder, and may actually decrease the
motion.
If all
of these attempts to improve your shoulder fail to give you a useable
shoulder, there are other more complex and involved procedures that
include tendon grafts and muscle transfers. These are rarely
necessary but will be discussed with you by your doctor if
necessary. Can
ROTATOR CUFF TEARS HEAL THEMSELVES? -- Does everyone need surgery?
Full
thickness rotator cuff tears generally do not heal or repair
themselves. Many people, however, have pain that goes away following a
rotator cuff tear. This is not because of healing, but because of
compensation by the remainder of the rotator cuff muscles that are not
torn, taking over the function of the muscle that is torn. For this
reason, not all people need to have rotator cuff tears fixed.
HOW IS
TENDINITIS OR “ROTATOR CUFF SYNDROME” TREATED?
Rotator
cuff syndrome (tendon or bursal pain without a full-thickness
tear) is extremely common and often responds to conservative measures.
Alternatives for treatment include anti-inflammatory medications by
mouth or injected cortisone into the space above the rotator
cuff. Of extreme importance, however, in treating rotator cuff syndrome
is physical therapy and home exercise programs designed to strengthen
the rotator cuff muscles.
These
exercises are not the type of exercises one ordinarily does at a gym or
with regular weight equipment. The reason that these exercises are
important is because strengthening of the rotator cuff will enable it to
function correctly, keeping the humeral head centered against the socket
of the shoulder joint. This will limit the rubbing that occurs between
the rotator cuff and the acromion above to prevent further irritation.
Other things that are often helpful in treating rotator cuff tendinitis
involve the use of hot or cold packs to decrease pain.
Additionally, if motion is limited, then stretching exercises are
also important.
If
rotator cuff tendinitis pain does not improve with these conservative
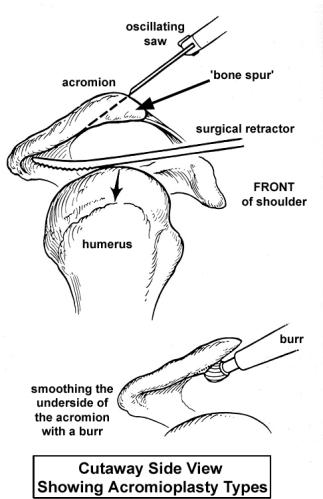
measures, surgical treatment may be indicated. The surgical treatment
for a tendinitis is known as acromioplasty or subacromial
decompression (see diagrams on next page). This can be done either
as an open procedure or as an arthroscopic procedure. During the
surgery, the bone spur that forms on the underside of the acromion is
removed and the acromion is smoothed, giving more space for the rotator
cuff when the shoulder is elevated.
(The upper diagram shows an
open acromioplasty, with an oscillating saw, and with a large
retractor holding down the humeral head. Arthroscopic acromioplasty
accomplishes the same goals, but only uses a rotary burr, as shown
in the lower diagram.
Impingement may not be the only problem in a shoulder that has begun to
show wear and tear due to aging and overuse. It is very common to see
degenerative (wear and tear) arthritis in the acromioclavicular (AC)
joint in addition to impingement. If there is reason to believe that an
arthritic acromioclavicular (AC) joint is contributing to the pain (most
do not), then the end of the clavicle may be removed as well. After
removal of about one half inch of the clavicle (not shown in this
handout), scar tissue fills the space left between the clavicle and the
acromion to form a false joint. The scar tissue that forms
creates a stable, flexible connection between the clavicle and the
scapula stopping the arthritic pain that was caused by bone rubbing
against bone. In most cases these procedures can be using the arthroscope. The arthroscope is a TV camera that is inserted into a joint through a small incision. Through other small incisions around the joint, the surgeon can insert special instruments to cut and burr away bone while he watches what he is doing on a TV screen. In a few cases, a larger open incision is made to allow removal of the bone. Usually an incision about 3 or 4 inches is made over the top of the shoulder. Bone spurs are removed and a part of the acromion is removed and smoothed by the surgeon. If necessary, the end of the clavicle is removed to perform the resection arthroplasty of the acromioclavicular (AC) joint. Recovery from shoulder surgery can be a slow process. Physical therapy will probably be needed for several weeks after your surgery. Getting the shoulder moving as fast as possible is important, but this must be balanced with the need to protect the healing muscles and tissues. You can expect the process of recovery to take several months.
HOW ARE
ROTATOR CUFF TEARS TREATED ?
Rotator
cuff tears are either acute, secondary to a trauma, or they are
chronic. Traumatic tears generally do better when surgically repaired
rather than with a trial of therapy first. Chronic tears generally are
best treated with a trial of therapy to see if the pain will resolve. If
not, they too are often candidates for operative repair.
Some
patients with chronic tears are not good candidates for repair because
the tear is too large or the rotator cuff muscles have already wasted
away, (atrophied).
For
those who do not get better with physical therapy, medications, or
injections for rotator cuff tears, repair of the rotator cuff may be
carried out either using an arthroscope or using an open procedure.
Surgery will usually be recommended the patient is young and very active
or if the tear causes continued weakness or pain. A subacromial
decompression (as described above) is also performed with rotator cuff
repair. The rotator cuff itself may be repaired back to the humeral head
using either sutures placed through bone or by using suture anchors.
Some
cuff tears can be fixed arthroscopically. Other tears are fixed by
making an incision (approximately 2-3 inches) over the outside of the
shoulder. (Your surgeon will determine which approach is best for the
particular tear)
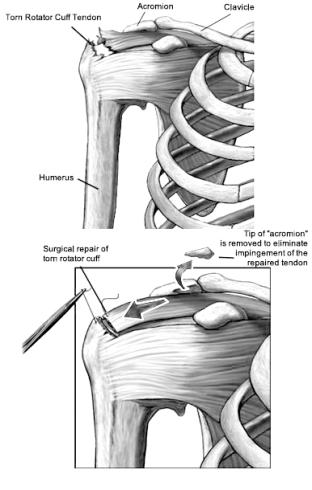
The
tears in the cuff are identified, and the torn edges are sutured
together and/or reattached to bone. This may require the placement of
drill holes, small screws or other anchors into the bone. These anchors
may be made of metal or a type of material that will dissolve over time.
Sometimes the tear is so large or the tissue so damaged that it is
impossible to completely fix. Bone from the acromion, the humeral head,
and the underside of the clavicle (collarbone) is often shaved and
removed to help reduce the pain after surgery.
Either
approach towards surgery can often be done as an outpatient procedure.
The
incision from the surgery will be closed with stitches and covered by a
sterile bandage. A ‘pain pump’ catheter may temporarily be left in the
shoulder to inject numbing medicine. You may have some swelling and
small bruises on your shoulder, but this should disappear within a few
days. For several weeks after your surgery, your arm will be placed into
a sling or harness that will immobilize the affected arm against the
body. Sometimes it is necessary to place a pillow or brace under the arm
for added support.
It will
take about 12 weeks for the tendon to heal completely. The early
recovery phase lasts approximately 6 weeks. During the first 4 - 6 weeks
you can and should use your hand, wrist, and elbow, but you should not
lift the shoulder with its own muscle until instructed to do so by your
doctor or therapist. Using the rotator cuff muscles too soon may cause
the repair to fail.
Using
the shoulder muscles for activities such as elevating the arm usually
starts at about 4 - 6 weeks after surgery. Your doctor may have you
begin an assisted physical therapy program to help you regain your
strength and range of motion. Full recovery from your surgery will take
9 - 12 months. Will a
rotator cuff repair relieve pain and
restore function? Pain relief is fairly reliable after a cuff repair. Increased strength and motion is not, and only occurs in about half of patients. Motion itself may even worsen following surgery, even if pain is gone.
HOW IS
PAIN CONTROLLED FOLLOWING SURGERY FOR THE ROTATOR CUFF?
For both
subacromial decompressions as well as repairs of the rotator cuff there
may be several different elements to anesthesia and pain control. One of
these is an injection in the nerves that go to the shoulder. This
injection is known as an intrascalene block and produces numbness
of the arm and the shoulder that may last several hours. This may be
done immediately prior to or during the time of surgery and will result
in a “numb arm” following the surgery, during which the patient feels no
pain.
Another
way to help the pain following rotator cuff surgery is through the
placement of a “pain pump”. A pain pump is a large syringe containing
a numbing medicine such as Marcaine that is then injected slowly and
continuously into the shoulder. The pain pump will provide numbing
medicine that will help, but not eliminate the pain from the surgery. It
is extremely important that the catheter for the pain pump be removed
when the medication is exhausted.
A third
way to help with pain following rotator cuff surgery is via medications
by mouth. Most of these are narcotics such as codeine or a synthetic
variant of codeine like Percocet. There is also the possibility to use
anti-inflammatory medicines to help control the pain or to use long
lasting medications such as OxyContin or MSContin. These three
approaches help control the pain following rotator cuff surgery.
WHAT
TYPE OF THERAPY FOLLOWS ROTATOR CUFF SURGERY?
For
patients that have subacromial decompressions without repair to the
rotator cuff, the main reason for therapy is to restore the motion of
the shoulder and strengthen the muscles of the shoulder. People who
have had this operation usually have no restrictions placed upon them as
motion of the shoulder cannot damage anything that was done during the
operation. As soon as their pain gets better, they find themselves
more able to perform regular daily activities and have better motion of
their shoulder. For most people that have subacromial decompressions, the pain from surgery is almost gone by week four and thereafter the patient will generally have less pain then they had before surgery. For the patients that have rotator cuff repairs, the physical therapy regimen is more restrictive. Because there is a repair of the rotator cuff to protect until the tendon actually heals to bone, the patient is not allowed to move his or her own shoulder using their own muscles for the first several weeks. A rehab protocol is outlined to the patient following surgery. The patient needs to be in a sling when not doing therapy for the first 6 weeks and no driving is permitted for the first 6 weeks. Starting at 6 weeks the patient can gradually start to raise their arm using his or her own muscles. Before this time, they need to be assisted by somebody else or with the aid of devices such as an overhead pulley or a cane.
Strengthening of the rotator cuff muscles following a rotator cuff
repair does not start until at least 12 weeks after surgery. Full
recovery from a rotator cuff repair may be anywhere from 6-12 months
following the surgery, although pain relief is often accomplished within
a few weeks after the surgery. CAN ALL ROTATOR CUFF SURGERY BE DONE ARTHROSCOPICALLY?
Arthroscopic surgery has improved rotator cuff treatment by providing a
less painful form of surgery for the patient. Many rotator cuff repairs
can be repaired arthroscopically. Other rotator cuff repairs are better
performed via a more traditional open surgery. The restrictions in use
of the shoulder after surgery are generally not different with an
arthroscopic or an open approach (unlike in general surgery where people
can do more sooner after laporoscopic surgery than after open
laporotomies). The reason for the restrictions is to protect the
repair, which heals at the same speed whether the skin incisions are
large or small. What
can go wrong with the surgery? For the vast majority of people, rotator cuff repair surgery has a good outcome, relieving pre-op pain. Complications occur in some, however. These complications can include and are not limited to problems with anesthesia, infections, re-tears, loss of motion, numbness in the arm, weakness, and arthritis. DO ROTATOR CUFF TEARS RECUR? While most people get good relief from repair of a rotator cuff tear, studies show that approximately one out of three large tears will reoccur. Fortunately, most of these people that have recurrent tears do not have pain associated with the recurrent tear. Because of this, repeat surgery is not usually needed. In some cases, however, a re-tear becomes very painful and may benefit from further surgical repair. Following a re-repair, the therapy protocol will be even more restricted and take a longer period of time.
|
|
|